

F.
Face
Look for an uneven smile or facial droop.
Above (from left to right): Joey English, M.D., Ph.D.; Lee Rink, R.N., Stroke Coordinator;
Matthew Deems,
Stryker Sales Representative; Nora Kasapligil, stroke survivor
As a third-year college student, Nora has a lot to live for, with hopes of traveling the world and helping others. But her dreams were put in jeopardy in June 2015 when she suffered an ischemic stroke. Nora is one of seven million stroke survivors in the U.S., but many are not as lucky as she was.
On the morning of her stroke, she had a severe headache, so went back to bed. An hour later, Nora got out of bed and walked straight into a wall. Dazed and confused, she went back to bed again. “I just didn’t understand what was going on.”
A short time later, when Nora’s roommate Christine checked in on her, wondering why she hadn’t gotten up for work, “[Nora] started repeating her words with really unclear sentences. She knew what she was trying to say, but it wasn’t getting out coherently.” Christine also noticed the left side of Nora’s body was swaying when she got up to walk. Suspecting Nora was having a stroke — a savvy understanding for someone so young — Christine called 911.
At the local hospital, the diagnosis of ischemic stroke — a large-vessel blockage of blood flow in the brain — was confirmed. By then, the left side of her body was paralyzed and she couldn’t speak. Unfortunately, Nora was not a candidate for tPA, the clot-busting drug that’s currently the only medical option for stroke. Her only chance for recovery was to have the clot removed with a stent retriever, a minimally invasive procedure that is now the standard of care for large-vessel blockages.

Left: Nora Kasapligil
and her roommate,
Christine Kubota
Look for an uneven smile or facial droop.
Is there weakness
in one arm?
Is speech slurred or jumbled?
Do not delay; call 911 immediately.

R&D Engineer Trevo
Nora was transferred to the California Pacific Medical Center in San Francisco, where they specialize in the procedure. Dr. Joey English, the Director of Neurointerventional Services, removed the clot using our Trevo retriever.
“The new stent retrieval devices for treating large-vessel occlusions are pretty remarkable advances,” says Dr. English. “I hate to think what Nora’s outcome would have been without this new technology. She’s living proof that Trevo has changed the way we treat stroke.”
The surgeon makes a small incision in the groin and, using a series of catheters, guides the device to the brain where it ensnares and then removes the clot through the catheter. The Trevo device provides full-length visibility for the surgeon, and therefore greater control and real-time information during its placement, integration and clot retrieval. In fact, it was the 2014 winner of the prestigious Prix Galien Award for best medical technology.
Led by R&D engineer Ryan Grandfield, the development of the Trevo retriever was several years in the making. “We had to figure out the intricate geometry so it could attach securely to everything from soft, jelly-like clots to hard ones,” Ryan explains. “It’s a nickel-titanium alloy with shape memory to help secure the clot.”
Within an hour of the procedure, Nora was able to move the left side of her body again; within a day her facial weakness and slurred speech were gone. “Everyone was so thrilled for her,” says Nora’s mother, Jill. “I will never live long enough to thank Christine and Dr. English.”
Only months after her stroke, with no residual symptoms, Nora is living independently with her roommate and is continuing her college studies. “When I see someone who’s had a stroke and I see that they have the symptoms I could have had, I think I’m really lucky.”
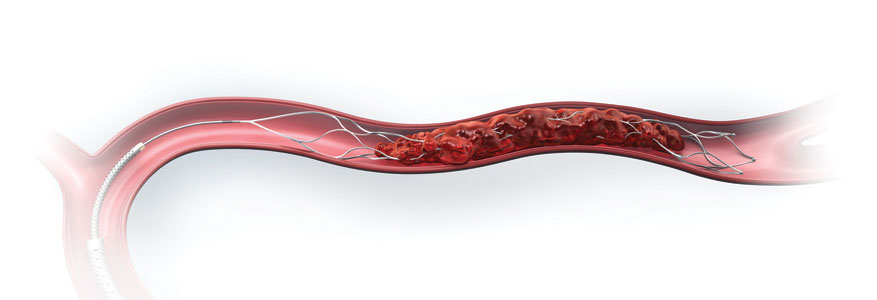
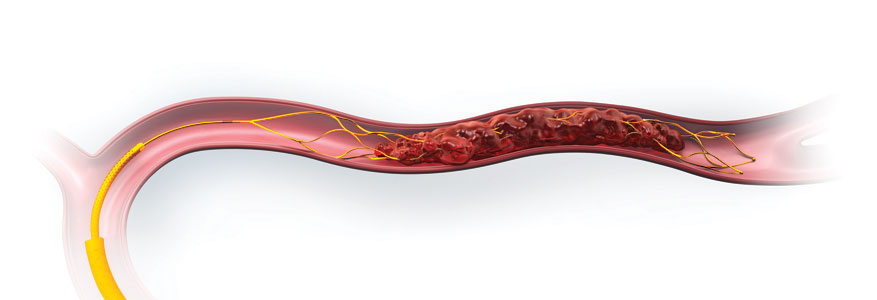
Stent retriever is attached to a wire and is designed to be retrieved with clot to open up the blocked artery
with it’s large, open cells
Dr. Joey English
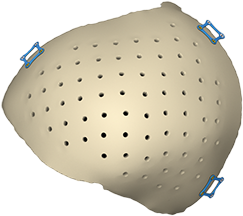
Director of Neurointerventional Services,Traditional methods of cranial reconstruction focus solely on the bone reconstruction of the skull and do not account for the overlying soft tissue that is an important factor in the overall cosmetic outcome of surgery. When the soft tissue is not addressed, it can lead to a visible deformity after the operation called PTH (persistent temporal hollowing).

When a surgeon removes a portion of the patient’s cranial bone to access the brain, the implant that is typically used diminishes blood supply. As a result, the overlying soft tissue is subject to atrophy or shrinkage. Our CCI Plus is a unique and patent-protected technology that accounts for both the bone reconstruction and the predicted soft tissue deficiency.
Our customized cranial implants are sent with a host bone model that is made using 3D printing technology, also known as additive manufacturing. The model is used to help orient the implant and allow the surgeon to “plan” the surgery prior to the actual operation.
This exclusive innovation is the result of a collaboration with craniofacial surgeon Chad Gordon, D.O., F.A.C.S., of Johns Hopkins Hospital. According to Dr. Gordon, “These implants provide, on average, 40 percent additional volume, which significantly decreases the need for surgical revisions and additional expense to the patient.”1
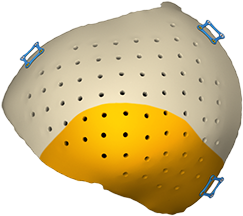
and also restore aesthetic symmetry by augmenting the temporal area of the skull to counter temporal hollowing.

The addition of our Mako Total Knee application to our market-leading Triathlon Knee System is a key milestone in reconstructive surgery. This new application expands the growth of robotic-arm assisted surgery in orthopaedics and has the potential to enhance both the surgeon and the patient experience.
Use of the Mako Total Knee application with our Triathlon Knee System will add to the company’s current robotic-arm assisted surgery portfolio of Partial Knee and Total Hip applications to provide a comprehensive solution in the robotic-arm assisted reconstructive service line.
We are launching a limited market release of the Mako Total Knee application in 2016, actively partnering with surgeons and experts to study the operating room workflow and learning curve. The observations from these studies will deliver valuable insights and data that will assist in defining the surgeon and staff training requirements and operating room configuration, which will enhance the user experience. This feedback will provide us with the opportunity to converge on a single workflow to allow every surgeon using the Mako Total Knee application the opportunity to reduce complexity and experience simpler and more reproducible procedures.


To date, more than 50,000 Mako Partial Knee and 10,000 Mako Total Hip procedures have been performed.2 As demand for knee and hip procedures continues to rise, Mako Robotic-Arm Assisted Systems are designed to enable surgeons to reduce variability within reconstructive procedures.3-13
The 1588 AIM platform with SDC3 1.5 Software allows surgeons to see and do more in minimally invasive surgery. The platform gives surgeons customized control of compatible surgical devices in the operating room, while enhancing visualization through five distinct imaging modalities.

Dr. Scott MelvinDirector of General Surgery at Montefiore Medical Center
“This new platform allows us to see critical anatomy in real time, with a simple touch of the button on the camera head,” said Dr. Scott Melvin, Director of General Surgery at Montefiore Medical Center. “The reality is that this technology brings a lot to the table,” said Dr. Santiago Horgan, Chief of Minimally Invasive Surgery at University of California, San Diego.
The five key elements of the platform include: IRIS (Infrared Illumination System), a visualization technology designed to reduce the risk of ureteral damage; ENV (Endoscopic Near Infrared Visualization), designed to reduce the risk of common bile duct injury during laparoscopy; Clarity, designed to improve anatomy visualization by enhancing tissue level detail and intrabody structures, which can improve image quality by up to 48 percent14; DRE (Dynamic Range Enhancement), designed to improve visualization in the surgical field by creating a brighter image in dark and posterior compartments; and Desaturation, which decreases the saturation of color in the image, a preference that varies by surgeon and specialty.
increase in image quality14


allows surgeons to see and do more in minimally invasive surgery. The platform gives surgeons customized control of compatible surgical devices in the operating room, while enhancing visualization through three distinct imaging modalities.
The signature portfolio represents the most comprehensive high-speed drill launch in Stryker’s 75-year history, the result of a close collaboration with surgeons to create an array of refined motors, attachments and cutting accessories that meet functional and ergonomic needs.

In fact, the collaboration created four new motors, four new attachment lines and more than 60 new cutting accessories for cranial and spine surgeries, and any number of other demanding and delicate procedures.
Since surgeons are always looking to improve performance, the signature portfolio provides multiple customization components, including 30 meticulously crafted attachments and many cutting accessories. Surgeons can also calibrate Stryker’s I.D. Touch software on the CORE Console to tailor how the electric drill will perform.
In essence, surgeons can select the drill they want, dial in how they want their electric drill to feel, and store their preferences in the ancillary CORE Console power source. Once selections are made, each surgeon can be confident that the drill will perform the way he or she wants — every time.













